Immunobiology: The Immune System in Health and Disease By Janeway Charles A, Paul Travers, Mark Walport, and Mark J Shlomchik With an introduction by Walter Sorochan
Posted December 11, 2021.
Introduction to immunity By Walter Sorochan
The Communicable Disease Center encourages everyone to get COVID vaccines and
booster shot as well. But millions of people are reluctant to do so. Why are
they reluctant to get a vaccine? What is the problem?
Many feel it is their right not to be vaccinated. Others do not believe that
the vaccines will not prevent getting infected; indeed, these are part of the thousands
who have died! Research author Walter Sorochan believes that the majority of
Americans do not understand how their body immune system works. If they did
understand how the covid vaccine is made, then they may be more prone to get
vaccinated. The federal government has done a terrible job of informing people
about all of this. The purpose of this article is to provide scientific
information about how the human body immune system works.
The immune system is complex.
The immune system is a collaborative effort by the entire body to maintain the
blood in a "clean" state; the result is immunity --- that is to say; an ability
by the body to protect itself from foreign invasion by organisms or substances
that might compromise it.Immune theory & dig sys
Immunity is medical term that describes a state of having sufficient biological defenses to avoid infection, disease, or other unwanted biological invasion. Immunity involves both specific and non-specific components.
The non-specific components act either as barriers or as eliminators of pathogens to stop infection by micro-organisms before they can cause disease. Other components of the immune system adapt themselves to each new disease encountered and are
able to generate pathogen-specific immunity
We have been told that it is the bones and lymphatic system, white blood cells, macrophages and T-cells makeup the
immune system and are the major protectors of the body. But as the illustration below shows, there are many body
organs involved in the immune system. The major organ not included in
the illustration is the colon and it's bacteria.
Immunity Types
Immunity to a disease is achieved through the presence of antibodies to that disease in a person’s system. Antibodies are proteins produced by the body to neutralize or destroy toxins or disease-carrying organisms.
Antibodies are disease-specific. For example, measles antibody will protect a person who is exposed to measles disease but will have no effect if he or she is exposed to mumps.
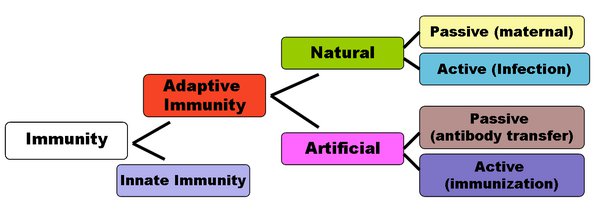
There are two types of immunity: active and passive:
Active Immunity results when exposure to a disease organism triggers the immune system to produce antibodies to that disease. Active immunity can be acquired through natural immunity or vaccine-induced immunity.
Natural immunity is acquired from vaccination of killed or weakened form of disease
Vaccine-induced immunity is acquired from vaccination with killed or weakened form of a disease.
Passive immunity occurs when a person is given antibodies to a disease rather than producing them through his or her own immune system.
A newborn baby acquires passive immunity from its mother through the placenta.
People can also get passive immunity through antibody-containing blood products such as immune globulin, which may be given when immediate protection from a specific disease is needed.
The major advantage to passive immunity is that protection is immediate, whereas active immunity takes time (usually several weeks) to develop
but is long-lasting. However, passive
immunity lasts only for a few weeks or months.
Vaccine-induced immunity is acquired through the introduction of a killed or
weakened form of the disease organism through vaccination.
Either way, if an
immune person comes into contact with that disease in the future, their immune
system will recognize it and immediately produce the antibodies needed to fight
it. Active immunity is long-lasting, and sometimes life-long.
Natural immunity occurs through contact with a disease causing agent; when
the contact is not deliberate, whereas artificial immunity develops only through
vaccinations. Both natural and artificial immunity can be further subdivided, depending on the amount of time the protection lasts. Passive immunity is short lived, and usually lasts only a few months, whereas protection via active immunity lasts much longer,
nd is sometimes life-long. The diagram below summarizes these divisions of immunity.
Herd immunity is a form of protection that occurs when people in a community become immune to a disease,” Dr. Evans says. “Herd immunity protects the individual and everyone else in the
community.”
The basic idea is that if enough people in a single community, or “herd,” have the antibodies needed to protect against a particular disease, that disease will have a hard time spreading from person to person. This is important because some people in the
community are especially susceptible to diseases, such as babies and young children, the elderly and those with compromised immune systems.
Herd immunity only works if enough of the population is vaccinated [like 80+
percent or more], either through previous infection or vaccination. It’s easy to assume that everyone else has antibodies, so it doesn’t matter if you receive a vaccine or not. But when enough people make this type of assumption, the community as a whole
will struggle to reach the herd immunity threshold, leaving space for infectious disease to continue spreading through the population.
Some persons may not be vaccinated, may be infected and display no symptoms
[asymptomatic] but still be able to infect others. This is what may be happening with coronavirus in United States.
Colon bacteria can determine level of immunity: Researchers since 2000 have discovered that there are over 400 good and bad bacteria living in the large intestine or colon. If the normal
balance of 80 - 85% good and 15 - 20 % bad bacteria is disrupted, then the bad bacteria multiply and can cause many of our illnesses and diseases. Today, most of us show the reverse ratio
or that of 80% bad and 20% good bacteria. Thus, it’s no coincidence that the
incidences of chronic and degenerative diseases have multiplied dramatically
since World War II. Affluence has provided a meat and potatoes, cheeseburger,
French fries, coke and junk diet that also feeds the colon bacteria that
dramatically lower the immune system. This makes most persons susceptible to infection and chronic diseases
and especially viruses.
Most important, the immune system is compromised! The most
compelling evidence comes from Dr. Michael D. Gershon, chairman of the
Department of anatomy and cell biology at Columbia University, in his book "The
Second Brain," published in 1999. Gershon: The second
brain
So how does the body keep the bacteria in the colon under control and the
immune system high? The answer is food that feeds both your body and the
bacteria in the colon.
People who love to eat what is referred to as comfort food --- like milk shakes,
soft drinks, white breads, white pastas, cookies, sweets, fries and hamburgers,
promote the growth of disease-causing bacteria in the colon that cause a low immune system.
Walker: Cure for Crohns DiseaseEwers: Inflammation
We need to make wiser food choices to improve the immune system and have
natural body immunity against viruses. Vaccines are of secondary importance. This
is what the federal government is not telling people. We should be focusing on
changing from the Standard American Diet [SAD] to eating more vegetables and
fruit and also testing the
immune level of people before vaccinating them. This is not being done!
What is immune system; By Bruce Lipton : Length = 32:42 mns.
If you want more specific information about immunity, then
you should read the medical version below:
The cells of theimmune
systemoriginate in the
bone
marrow, where many of them also mature. They then migrate to guard
the peripheral tissues, circulating in the blood and in a specialized
system of vessels called thelymphatic
system.
1-1. The white blood cells of the immune system derive from precursors in the bone marrow
All the cellular elements of blood,
including the red blood cells that transport oxygen, the platelets
that trigger blood clotting in damaged tissues, and the white blood
cells of theimmune
system, derive ultimately from the sameprogenitoror
precursor cells—thehematopoietic
stem cellsin the bone marrow. As these stem cells can give rise to all of the
different types of blood cells, they are often known as pluripotent
hematopoietic stem cells. Initially, they give rise to stem cells of
more limited potential, which are the immediate progenitors of red
blood cells, platelets, and the two main categories of white blood
cells. The different types of blood cell and their lineage
relationships are summarized inFig.
1.3. We shall be concerned here with all the cells derived from
the common lymphoid progenitor and the myeloid progenitor, apart
from the megakaryocytes and red blood cells.
Figure 1.3 All the cellular elements of blood, including
the lmphocytes of the adaptive immune system, arise from hematopoietic stem cells in the bone marrow. These pluripotent cells divide to produce two more specialized types of stem cells, a common lymphoid.
(more...)
Themyeloid
progenitoris the precursor of the granulocytes,
macrophages, dendritic cells, and mast cells of theimmune
system.Macrophagesare
one of the three types of phagocyte in the immune system and are
distributed widely in the body tissues, where they play a critical
part ininnate
immunity. They are the mature form of monocytes, which circulate
in the blood and differentiate continuously into macrophages upon
migration into the tissues. Dendritic
cellsare specialized to take upantigenand
display it for recognition by
lymphocytes.
Immature dendritic cells migrate from the blood to reside in the
tissues and are both phagocytic and macropinocytic, ingesting large
amounts of the surrounding extracellular fluid. Upon encountering a
pathogen, they rapidly mature and migrate to lymph nodes.
Mast cells, whose blood-borne precursors are not well defined,
also differentiate in the tissues. They mainly reside near small
blood vessels and, when activated, release substances that affect
vascular permeability. Although best known for their role in
orchestrating allergic responses, they are believed to play a part
in protecting mucosal surfaces against pathogens.
The granulocytes are so called
because they have densely staining granules in their cytoplasm; they
are also sometimes called polymorphonuclear leukocytes because of
their oddly shaped nuclei. There are three types of granulocyte, all
of which are relatively short lived and are produced in increased
numbers during immune responses, when they leave the blood to
migrate to sites of infection or inflammation.Neutrophils,
which are the third phagocytic cell of theimmune
system, are the most numerous and most important cellular
component of the innateimmune
response: hereditary deficiencies in neutrophil function lead to
overwhelming bacterial infection, which is fatal if untreated.Eosinophilsare
thought to be important chiefly in defense against parasitic
infections, because their numbers increase during a parasitic
infection. The function of basophils is probably similar and
complementary to that of eosinophils and mast cells; we shall
discuss the functions of these cells in Chapter 9 and their role in
allergic inflammation in Chapter 12. The cells of the myeloid
lineage are shown inFig. 1.4.
Figure 1.4
Myeloid cells in innate and adaptive immunity. Cells of the myeloid lineage perform various important functions in the immune response.
The cells are shown schematically in the
left column in the form in which they will be represented throughout the rest(more...)
Thecommon
lymphoid progenitorgives rise to thelymphocytes,
with which most of this book will be concerned. There are two major
types of lymphocyte: B lymphocytes or B cells, which when activated
differentiate into plasma cells that secrete antibodies; andT
lymphocytesorT
cells, of which there are two main classes. One class
differentiates on activation intocytotoxic
T cells, which kill cells infected with viruses, whereas the
second class of T cells differentiates into cells that activate
other cells such as B cells and macrophages.
Mostlymphocytesare
small, featureless cells with few cytoplasmic organelles and much of
the nuclear chromatin inactive, as shown by its condensed state (Fig.
1.5). This appearance is typical of inactive cells and it is not
surprising that, as recently as the early 1960s, textbooks could
describe these cells, now the central focus of immunology, as having
no known function. Indeed, these small lymphocytes have no
functional activity until they encounterantigen,
which is necessary to trigger their proliferation and the
differentiation of their specialized functional characteristics.
Figure 1.5
Lymphocytes are mostly small and in active cells. The left
panel shows a light micrograph of a small lymphocyte
surrounded by red blood cells.
Note the condensed chromatin
of the nucleus, indicating little trans-criptional activity,
the relative absence(more...)
Lymphocytes are remarkable in being
able to mount a specificimmune
responseagainst virtually any foreignantigen.
This is possible because each individual lymphocyte matures bearing
a unique variant of a prototype antigen receptor, so that the
population of T and B
lymphocytescollectively
bear a huge repertoire of receptors that are highly diverse in their
antigen-binding sites. TheB-cell
antigen receptor(BCR)
is a membrane-bound form of the
antibodythat
theB
cellwill secrete after activation and
differentiation to plasma cells. Antibody molecules as a class are
known asimmunoglobulins,
usually shortened toIg,
and the antigen receptor of B lymphocytes is therefore also known asmembrane
immunoglobulin(mIg).
TheT-cell
antigen receptor(TCR)
is related to immunoglobulin but is quite distinct from it, as it is
specially adapted to detect antigens derived from foreign proteins
or pathogens that have entered into host cells. We shall describe
the structures of these lymphocyte
antigen
receptorsin detail in Chapters 3, 4, and 5, and
the way in which their diversity of binding sites is created as
lymphocytes develop in Chapter 7.
A third lineage of lymphoid cells,
called natural killer cells, lack antigen specific receptors and are
part of the innateimmune
system. These cells circulate in the blood as large
lymphocytes with
distinctive cytotoxic granules (Fig.
1.6). They are able to recognize and kill some abnormal cells,
for example some tumor cells and virus-infected cells, and are
thought to be important in the innate immune defense against
intracellular pathogens.
Figure 1.6
Natural killer (NK) cells. These are large granular
lymphocyte-like cells with important functions in innate
immunity. Although lacking
antigen-specific receptors, they
can detect and attack certain virus-infected cells.
Photograph courtesy of N. Rooney (more...)
1-2. Lymphocytes mature in the bone marrow or the thymus
The lymphoid organs are organized
tissues containing large numbers of
lymphocytes in
a framework of nonlymphoid cells. In these organs, the interactions
lymphocytes make with nonlymphoid cells are important either to
lymphocyte development, to the initiation of adaptive immune
responses, or to the sustenance of lymphocytes.
Lymphoid
organs can be divided broadly into central or
primary lymphoid organs, where lymphocytes are generated, and
peripheral or secondary
lymphoid organs, where adaptive immune responses are initiated
and where lymphocytes are maintained. The central lymphoid organs
are the bone
marrow and the thymus,
a large organ in the upper chest; the location of the thymus, and of
the other lymphoid organs, is shown schematically in Fig.
1.7.
Figure 1.7
The distribution of lymphoid tissues in the body.
Lymphocytes arise from stem cells in bone marrow, and
differentiate in the central lymphoid organs (yellow), B
cells in bone marrow and T cells in the thymus. They migrate
from these tissues and are carried (more...)
Both B and T
lymphocytes originate in the bone
marrow but only B lymphocytes mature there; T
lymphocytes migrate to the thymus to
undergo their maturation. Thus B lymphocytes are so-called because
they are bone marrow derived, and T lymphocytes because they are
thymus derived. Once they have completed their maturation, both
types of lymphocyte enter the bloodstream, from which they migrate
to the peripheral lymphoid organs.
1-3. The peripheral lymphoid organs are specialized to trap antigen,
to allow the initiation of adaptive immune responses, and to provide
signals that sustain recirculating lymphocytes
Pathogens can enter the body by
many routes and set up an infection anywhere, but
antigen and lymphocytes will
eventually encounter each other in the peripheral lymphoid
organs—the lymph nodes, the spleen,
and the mucosal lymphoid tissues (see Fig.
1.7). Lymphocytes are continually recirculating through these
tissues, to which antigen is also carried from sites of infection,
primarily within macrophages and dendritic cells. Within the
lymphoid organs, specialized cells such as mature dendritic cells
display the antigen to lymphocytes.
The lymph nodes are highly
organized lymphoid structures located at the points of convergence
of vessels of the lymphatic
system, an extensive system of vessels that collects
extracellular fluid from the tissues and returns it to the blood.
This extracellular fluid is produced continuously by filtration from
the blood, and is called lymph. The vessels are lymphatic vessels or lymphatics (see Fig.
1.7). Afferent
lymphatic vessels drain fluid from the tissues and
also carry antigen-bearing
cells and antigens from infected tissues to the lymph nodes, where
they are trapped. In the lymph nodes, B
lymphocytes are
localized in follicles,
with T
cells more diffusely distributed in surrounding
paracortical areas, also referred to as T-cell
zones. Some of the B-cell follicles include germinal centers,
where B cells are undergoing intense proliferation after
encountering their specific antigen and their cooperating T cells (Fig.
1.8). B and T
lymphocytes are segregated in a similar fashion in
the other peripheral lymphoid tissues, and we shall see that this
organization promotes the crucial interactions that occur between B
and T cells upon encountering antigen.
Figure 1.8 Organization of a lymph node. As shown in the
diagram on the left, a lymph node consists of an outermost
cortex and an inner medulla.
The cortex is composed of an
outer cortex of B cells organized into lymphoid follicles,
and deep, or aracortical, areas (more...)
The spleen is
a fist-sized organ just behind the stomach (see Fig.
1.7) that collects antigen from
the blood. It also collects and disposes of senescent red blood
cells. Its organization is shown schematically in Fig.
1.9. The bulk of the spleen is composed of red
pulp, which is the site of red blood cell disposal. The lymphocytes surround
the arterioles entering the organ, forming areas of white
pulp, the inner region of which is divided into a periarteriolar
lymphoid sheath (PALS),
containing mainly T
cells, and a flanking B-cell
corona.
Figure 1.9
Organization of the lymphoid tissues of the spleen. The
schematic at top right shows that the spleen consists of red
pulp (pink areas in the top panel),
which is a site of red
blood cell destruction, interspersed with lymphoid white
pulp. An enlargement of (more...)
The gut-associated
lymphoid tissues (GALT),
which include the tonsils,
adenoids,
and appendix,
and specialized structures called Peyer's patches in the small
intestine, collect antigen from
the epithelial surfaces of the gastrointestinal tract. In Peyer's
patches, which are the most important and highly organized of these
tissues, the antigen is collected by specialized epithelial cells
called multi-fenestrated or M
cells. The lymphocytes form
a follicle consisting of a large central dome of B lymphocytes
surrounded by smaller numbers of T
lymphocytes (Fig.
1.10). Similar but more diffuse aggregates of lymphocytes
protect the respiratory epithelium, where they are known as bronchial-associated
lymphoid tissue (BALT),
and other mucosa, where they are known simply as mucosal-associated
lymphoid tissue (MALT).
Collectively, the mucosal immune
system is estimated to contain as many lymphocytes
as all the rest of the body, and they form a specialized set of
cells obeying somewhat different rules.
Figure 1.10 Organization of typical gut-associated
lymphoid tissue. As the diagram on the left shows, the bulk of the tissue is B
cells, organized
in a large and highly active domed follicle. T cells occupy the areas between follicles. The antigen enters across a specialized
(more...)
Although very different in
appearance, the lymph nodes, spleen,
and mucosal-associated lymphoid tissues all share the same basic
architecture. Each of these tissues operates on the same principle,
trapping antigen from
sites of infection and presenting it to migratory small lymphocytes,
thus inducing adaptive immune responses. The peripheral lymphoid
tissues also provide sustaining signals to the lymphocytes that do
not encounter their specific antigen, so that they continue to
survive and recirculate until they encounter their specific antigen.
This is important in maintaining the correct numbers of circulating
T and B lymphocytes, and ensures that only those lymphocytes with
the potential to respond to foreign antigen are sustained.
1-4. Lymphocytes circulate between blood and lymph
Small B and T
lymphocytes that have matured in the bone
marrow and thymus but
have not yet encountered antigen are
referred to as naive lymphocytes. These cells circulate continually
from the blood into the peripheral lymphoid tissues, which they
enter by squeezing between the cells of capillary walls. They are
then returned to the blood via the lymphatic vessels (Fig.
1.11) or, in the case of the spleen,
return directly to the blood. In the event of an infection,
lymphocytes that recognize the infectious agent are arrested in the
lymphoid tissue, where they proliferate and differentiate into effector
cells capable of combating the infection.
Figure 1.11
Circulating lymphocytes encounter antigen in peripheral
lymphoid organs. Naive lymphocytes recirculate constantly
through
peripheral lymphoid tissue, here illustrated as a
lymph node behind the knee, a popliteal lymph node. Here,
they may encounter their (more...)
When an infection occurs in the
periphery, for example, large amounts of antigen are
taken up by dendritic cells which then travel from the site of
infection through the afferent lymphatic vessels into the draining
lymph nodes (see Fig.
1.11). In the lymph nodes, these cells display the antigen to
recirculating T
lymphocytes, which they also help to activate. B cells that
encounter antigen as they migrate through the lymph node are also
arrested and activated, with the help of some of the activated T
cells. Once the antigen-specific lymphocytes have undergone a
period of proliferation and differentiation, they leave the lymph
nodes as effector cells through the efferent
lymphatic vessel (see Fig.
1.8).
Because they are involved in
initiating adaptive immune responses, the peripheral lymphoid
tissues are not static structures but vary quite dramatically
depending upon whether or not infection is present. The diffuse
mucosal lymphoid tissues may appear in response to infection and
then disappear, whereas the architecture of the organized tissues
changes in a more defined way during an infection. For example, the
B-cell follicles of
the lymph nodes expand as B lymphocytes proliferate
to form germinal centers (see Fig.
1.8), and the entire lymph node enlarges, a phenomenon
familiarly known as swollen glands.
Summary
Immune responses are mediated by
leukocytes, which are derived from precursors in the bone
marrow. A pluripotent hematopoietic stem cell gives rise to the lymphocytes responsible
for adaptive immunity, and also to myeloid lineages that participate
in both innate and adaptive immunity. Neutrophils,
eosinophils, and basophils are collectively known as granulocytes;
they circulate in the blood unless recruited to act as effector
cells at sites of infection and inflammation. Macrophages and
mast cells complete their differentiation in the tissues where they
act as effector cells in the front line of host defense and initiate
inflammation. Macrophages phagocytose bacteria,
and recruit other phagocytic cells, the neutrophils, from the blood. Mast
cells are exocytic and are thought to orchestrate
the defense against parasites as well as triggering allergic
inflammation; they recruit eosinophils and basophils, which are also
exocytic. Dendritic
cells enter the tissues as immature phagocytes
where they specialize in ingesting antigens. These antigen-presenting
cells subsequently migrate into lymphoid tissue. There are two major
types of lymphocyte: B lymphocytes, which mature in the bone marrow;
and T
lymphocytes, which mature in the thymus.
The bone marrow and thymus are thus known as the central or primary
lymphoid organs. Mature lymphocytes recirculate continually from the
bloodstream through the peripheral or secondary lymphoid organs,
returning to the bloodstream through the lymphatic vessels. Most
adaptive immune responses are triggered when a recirculating T cell
recognizes its specific antigen on the surface of a dendritic cell.
The three major types of peripheral lymphoid tissue are the spleen,
which collects antigens from the blood; the lymph nodes, which
collect antigen from sites of infection in the tissues; and the
mucosal-associated lymphoid tissues (MALT),
which collect antigens from the epithelial surfaces of the body.
Adaptive immune responses are initiated in these peripheral lymphoid
tissues: T
cells that encounter antigen proliferate and
differentiate into antigen-specific effector cells, while B cells
proliferate and differentiate into antibody-secreting
cells.
References
Janeway Charles A, Paul Travers, Mark Walport, and Mark J Shlomchik, Immunobiology, 5th edition The Immune System in Health and Disease, New York: Garland Science; 2001.
Janeway: Book Immune system in health & disease 2001